Case Study · Consumer Health
ClinCalc
Consumer health self-check & multimodal interpretation platform

Pain points
Many people get a lab report full of numbers and jargon and don't know which values are concerning and which can wait. The default behaviors are: Google it, ask family, or ignore. Two structural problems sit underneath:
- Information asymmetry — medical terminology is hostile to non-experts
- Privacy concerns — pasting lab values into ChatGPT isn't safe
System architecture
"Rules-first, then LLM" three-layer architecture: local interpretation → structured injection → LLM translation. Raw patient data never leaves the device.
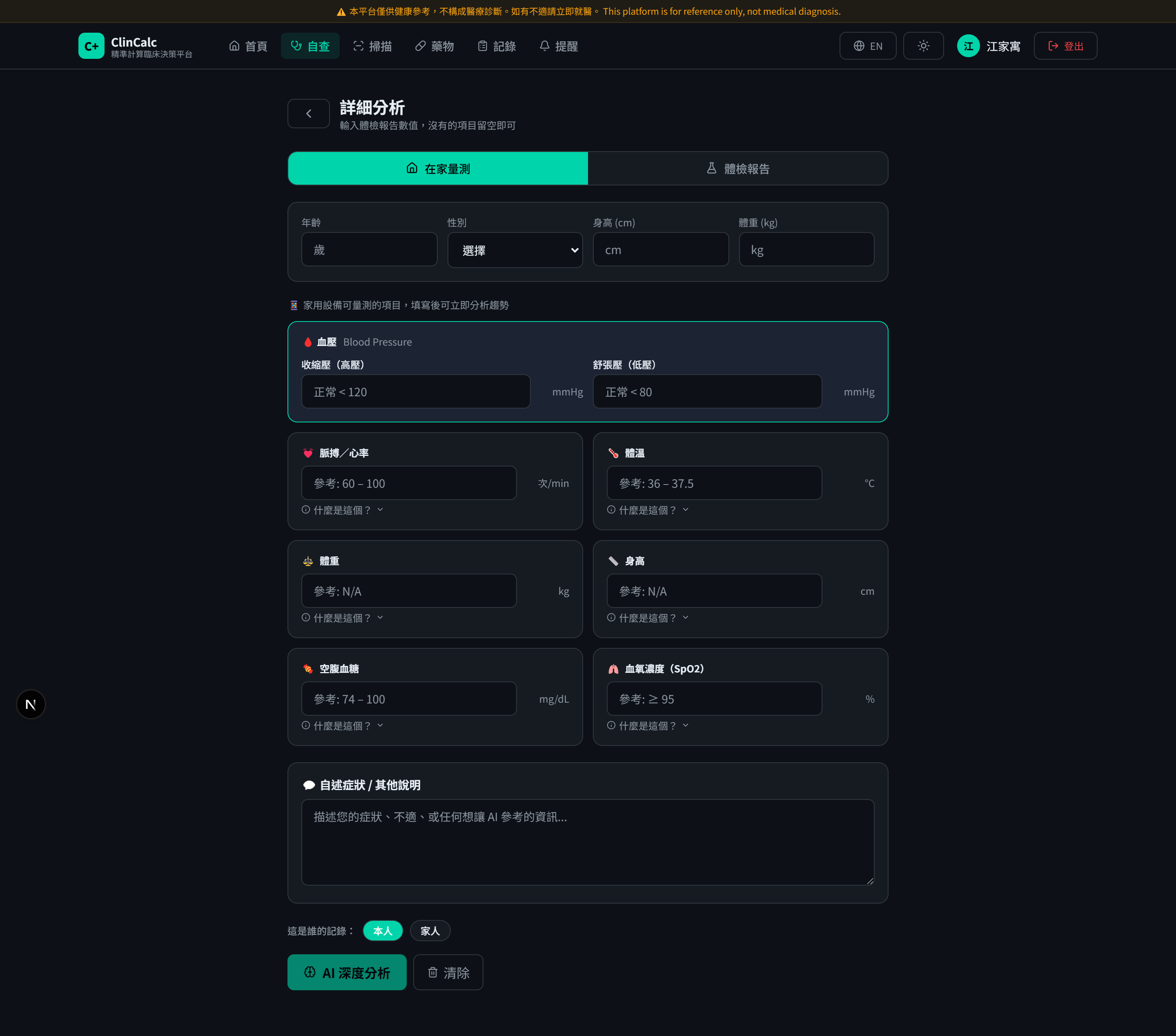
- 1 · User input
Enter 45 lab indicators, upload a lab-report photo, or click symptoms on the body map.
- 2 · In-browser local rules engine
Queries the
referenceRanges.tsknowledge base; each indicator is interpreted in real time as "normal / mildly high / mildly low / severely high / severely low". Raw values never leave the browser. - 3 · Cloudflare Worker (edge)
Receives the structured interpretation (not raw values), composes the Gemini prompt. Free tier 100K req/day is enough for expected traffic.
- 4 · Google Gemini 1.5 Flash
Translates medical terms, OCRs images. The LLM sees "CKD G3a" — not "Mr. Chiang's eGFR=45".
- 5 · Supabase (PostgreSQL + Auth)
User accounts, medication reminders, health record history — all protected by RLS.
Design highlight 1 — Rules first, then LLM
ClinCalc integrates Gemini using a "query the knowledge base first, then hand off to the
LLM" pattern: after the user fills in 45 indicators, the frontend looks up
referenceRanges.ts per field and calls checkAbnormal() for a 5-level
verdict, then composes the structured interpretation as the prompt to Gemini.
Gemini doesn't need to memorize each indicator's normal range — that reduces hallucination.
Trade-off
- Limited rule coverage: fuzzy holistic judgments ("how does my report look overall?") aren't handled by the rules engine, and the LLM is constrained from free generation → users feel "it doesn't do much"
- Knowledge base is manually maintained: upgrading from KDIGO 2012 to 2024 meant hand-editing the reference table
Design highlight 2 — Where multimodal models actually help
Gemini 1.5 Flash's multimodal capability is restricted to two well-defined "translation" tasks — never clinical decisions:
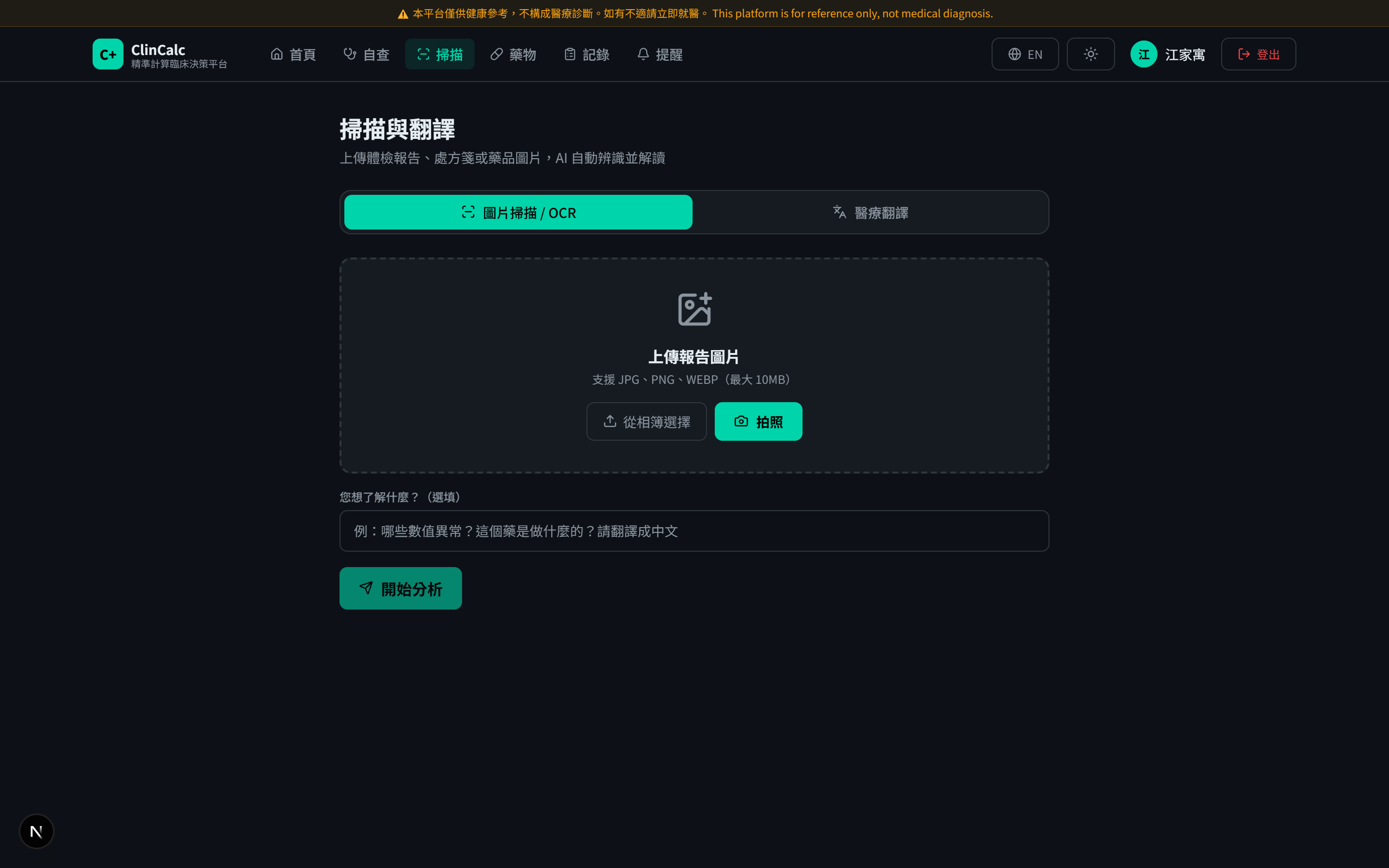

Trade-off
OCR accuracy on handwritten reports is still low (< 70%); translation occasionally misfires on uncommon abbreviations. The frontend validates citations from the model output and shows a "physician confirmation needed" tag on anomalies.
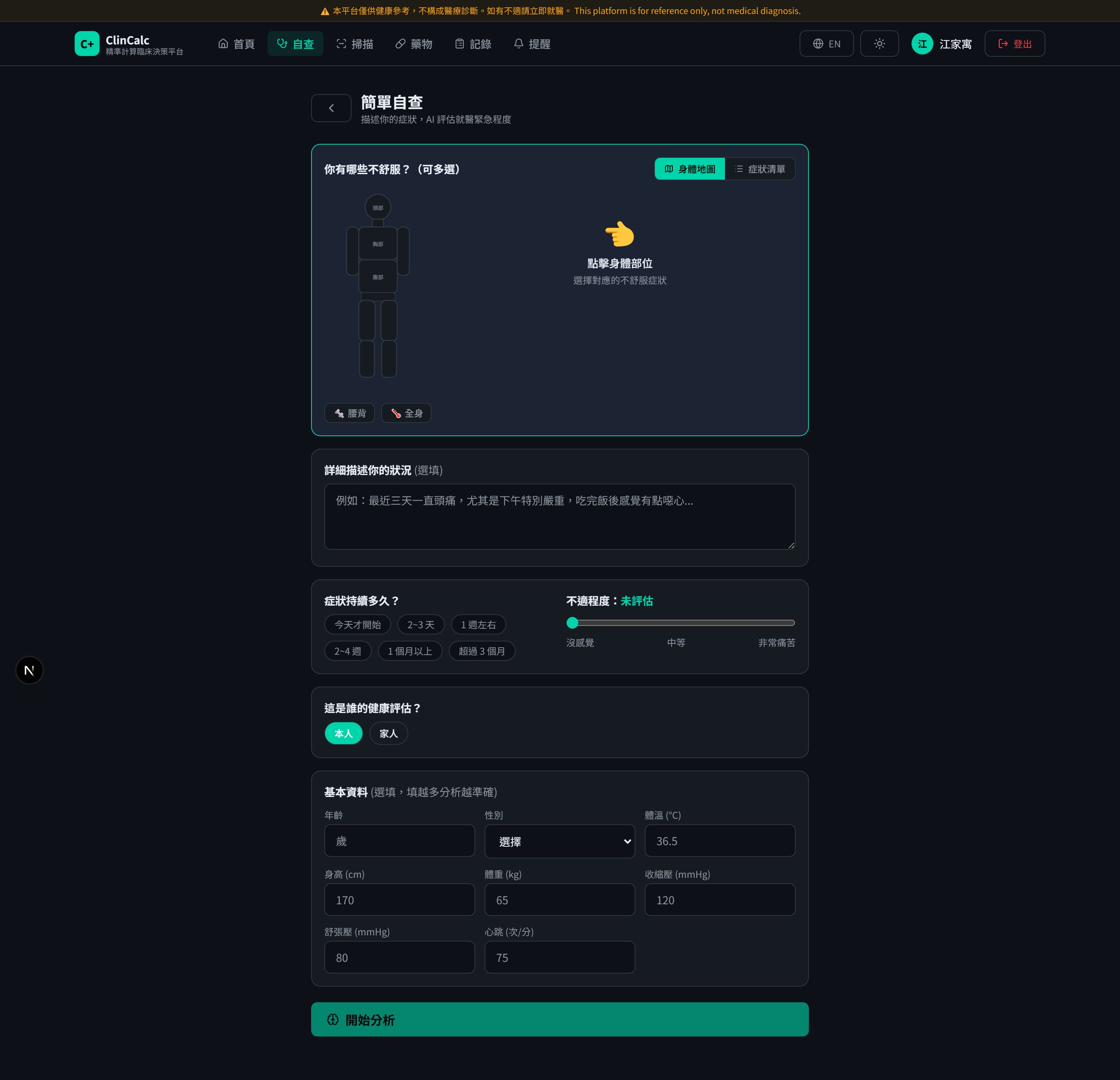
Design highlight 3 — Interactive symptom exploration
Conventional symptom search is keyword-typing. ClinCalc switches to a visual map: click a body region → expand common symptoms in that region → Gemini provides preliminary differential ranking and red-flag prompts.
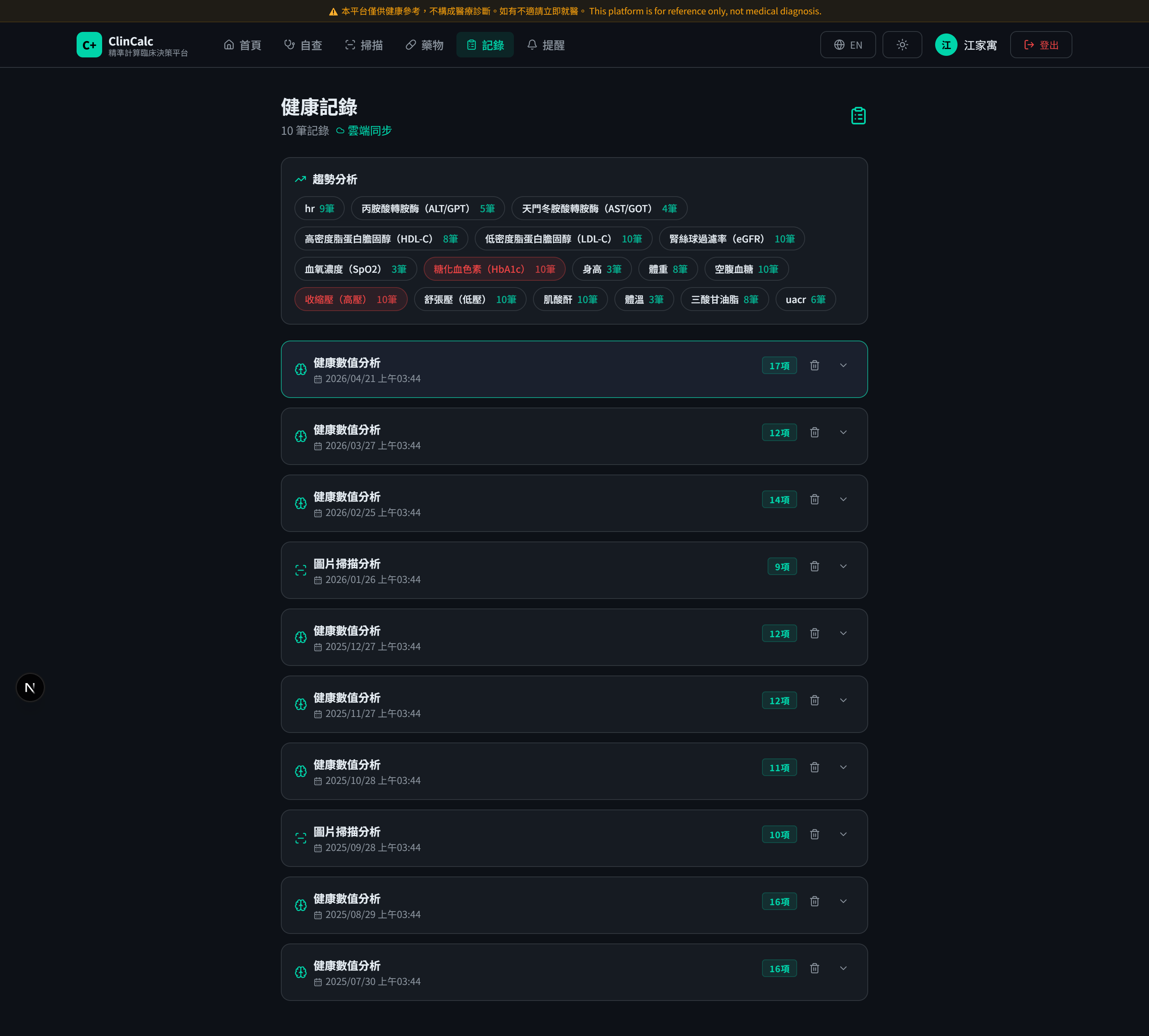
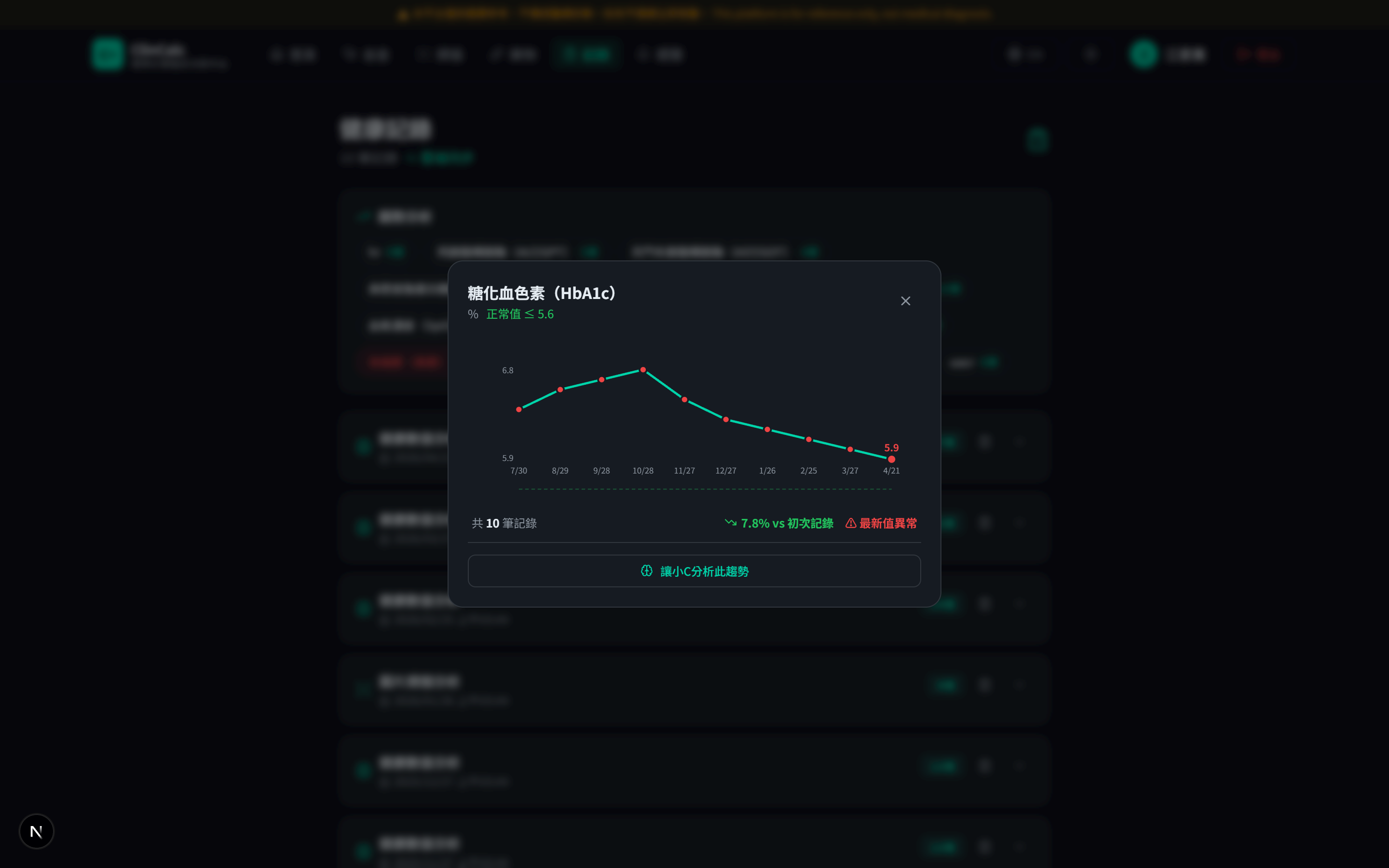
Derived feature: personal health tracking
After interpretation, the system stores results in Supabase (RLS-protected), forming a personal time series. Users can track 9-month trends per indicator, set medication reminders, and issue one-time tokens for a physician's temporary access.
Security & privacy design
Four layers of protection, browser → backend:
- Local-first computation
All 45-indicator interpretation logic and KDIGO staging compute entirely in the browser; raw lab values never leave the device. Only structured interpretations go to the backend.
- LLM only sees structured data
Gemini prompts contain only de-identified strings like "CKD G3a", never raw patient numbers. Reduces both hallucination risk and privacy risk.
- Storage-layer RLS isolation
User accounts, medication reminders, and health-record history live in Supabase, with PostgreSQL RLS on every table ensuring users can only read/write their own rows. Cross-account data won't leak even if the application layer is breached.
- Edge secret isolation + standard web security
Gemini API key and Supabase service-role key live only in Cloudflare Worker runtime secrets — never exposed to the frontend bundle. Combined with HTTPS only, Secret Scanning, Push Protection, and Dependabot for supply-chain defense.
Evaluation
The rules engine (KDIGO staging) was tested end-to-end: KDIGO 2024 international guideline cases as ground truth, compared against system output via confusion matrix and ROC curve.
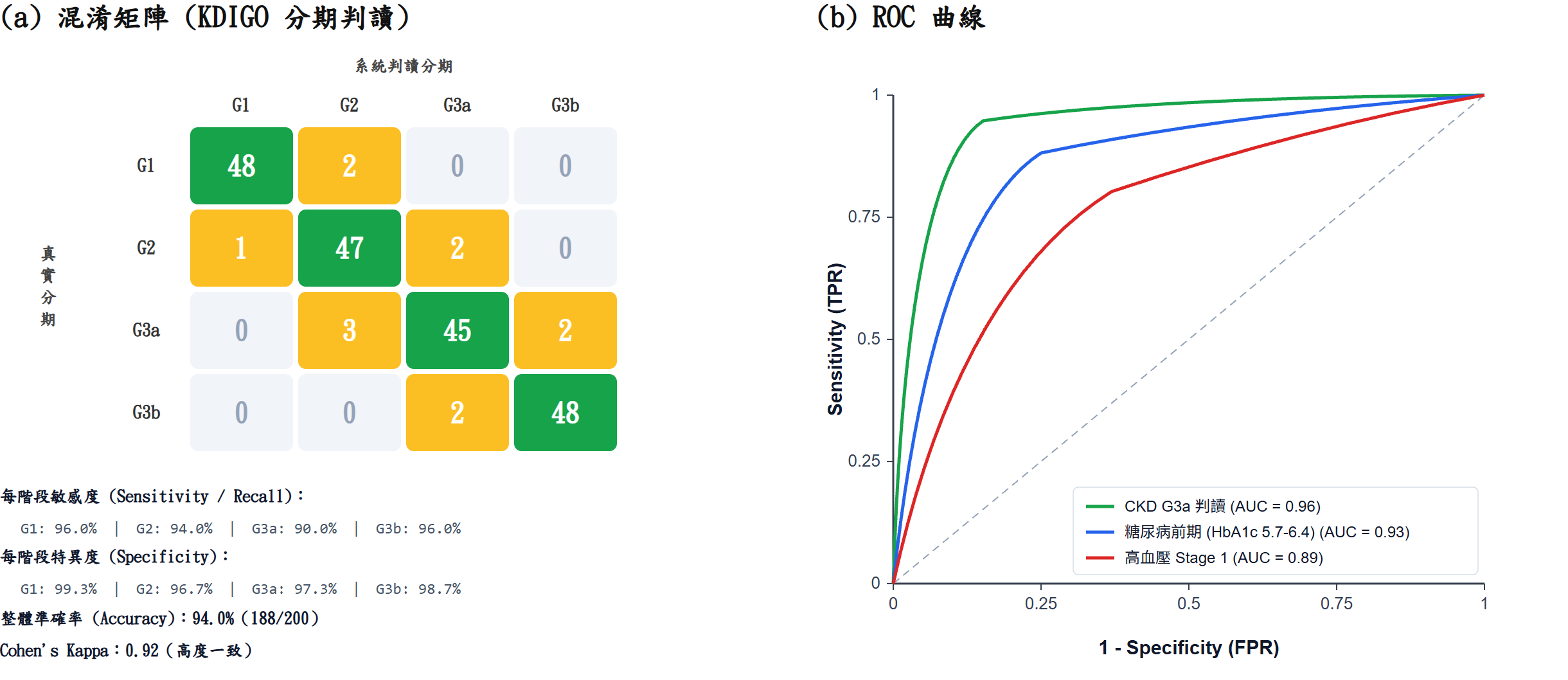
Note: this evaluation covers only the rules engine (not LLM output). Safety on the LLM side comes from structured injection + citation validation as preventive control; no public accuracy claim is made.
Tech stack
Research questions surfaced
- Can the "rules-first, then LLM" strategy generalize to fuzzy domains? The strategy works well on KDIGO staging, but rule coverage is insufficient for "holistic judgment" tasks. How do you design a graded "rules ↔ LLM" intervention ratio?
- How do clinical guideline updates propagate into a CDSS? KDIGO updates every few years; manually updating rule bases isn't sustainable. Could RAG turn clinical guidelines into a dynamic knowledge base?
- Limits of multimodal systems in non-expert user contexts — for users without medical training, how much algorithmic error is tolerable? How do you design disclosure and fallbacks?